What is a PRSB Standard?
Every time we interact with health or social care services, people make a record of what happens. Over a lifetime, this information forms our health and care history.
These pages explain what standards are and why we need them to record our health and care information in a consistent way so that it can be made available whenever it is needed, such as when we attend a hospital appointment or order medication from the pharmacy.
Why do we need information standards?
Our health and care information isn’t all recorded in a single system but in many different systems. When we go to hospital or to a GP surgery, a record of the conversation between the person and clinician is made, including any decisions and actions taken. Records are created in other settings too, such as care homes.
The fact is that people access care in many more settings today than ever before, and for professionals and people themselves to have a complete picture of a person’s health and care, we need to join all these many records together.

Recording information consistently
In health and care, agreed national standards and definitions must be used so that any system can share and interpret information consistently, preserving its meaning across services.

Right place, right time
When information is recorded consistently across different settings, it can be shared with the right professionals at the right time, supporting informed decisions about a person’s care.

Information tailored for different needs
Not everyone we interact with needs to see all the information in all these records to advise us on what tests we might need, or diagnose a condition, or meet our care and support needs, but they might need to see some information from more than one record.
Different types of information standards
Different types of information standards are needed for information to flow between computer systems.
Information record standards
PRSB standards are information record standards. They define the information needed in a person’s health and care record, such as their allergies, vaccinations and medications. They also include information that is important to the person, such as how best to communicate with them, how to help them feel at ease or details about how they like to take their medication.
Data and terminology standards
Terminology standards include SNOMED CT, a clinical vocabulary used for capturing clinical terms for example for diagnoses and treatments in electronic patient records. Find out more about SNOMED CT.
Data standards set out how information should be formatted such as birth date DD-MM-YYYY and what values (or codes) can be used; for example, Ethnic Categories, A (White – British) or M (Black or Black British – Caribbean).
Technical standards and specifications
Technical standards specify how information defined in a record standards is to be held or moved between systems. These can be based on Fast Healthcare Interoperability Resources (FHIR).
Application Programming Interfaces (APIs) are examples of technical standards that enable communication between two systems. Examples include FHIR UK Core APIs, Transfer of Care Inpatient Discharge – FHIR API (API catalogue – NHS Digital)
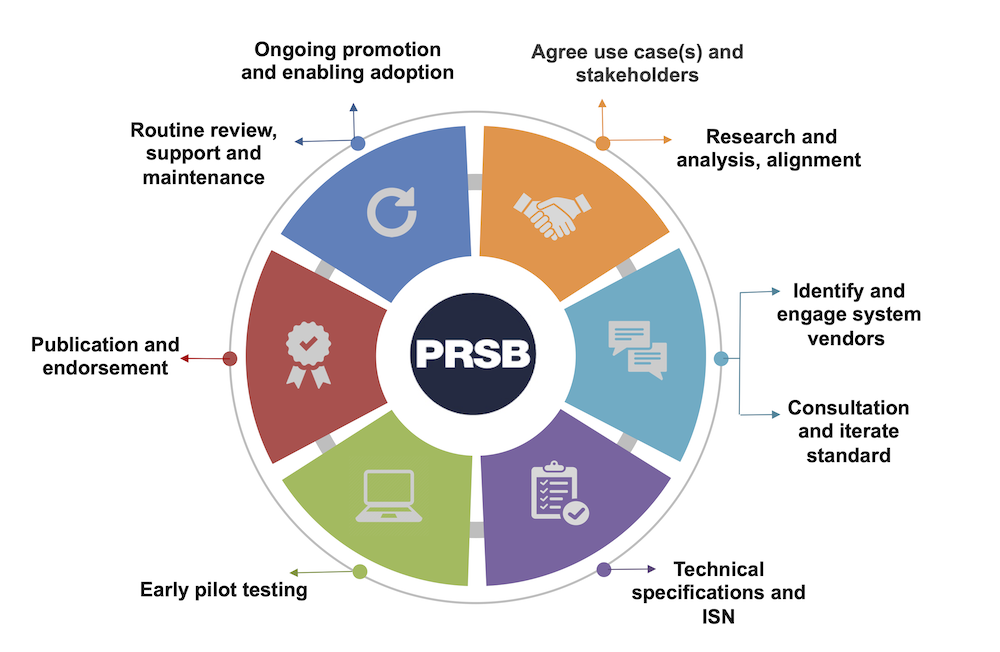
How do we create standards?
Early research ensures our work is evidence based, and then developed through consultation with our members and other relevant stakeholders, focusing on frontline staff and people who use the services.
Everyone agrees what information should be recorded at any stage of a person’s treatment to ensure high quality care can be provided. It also means that IT systems can be designed to share and retrieve the relevant information when it is needed across multiple services and care settings.